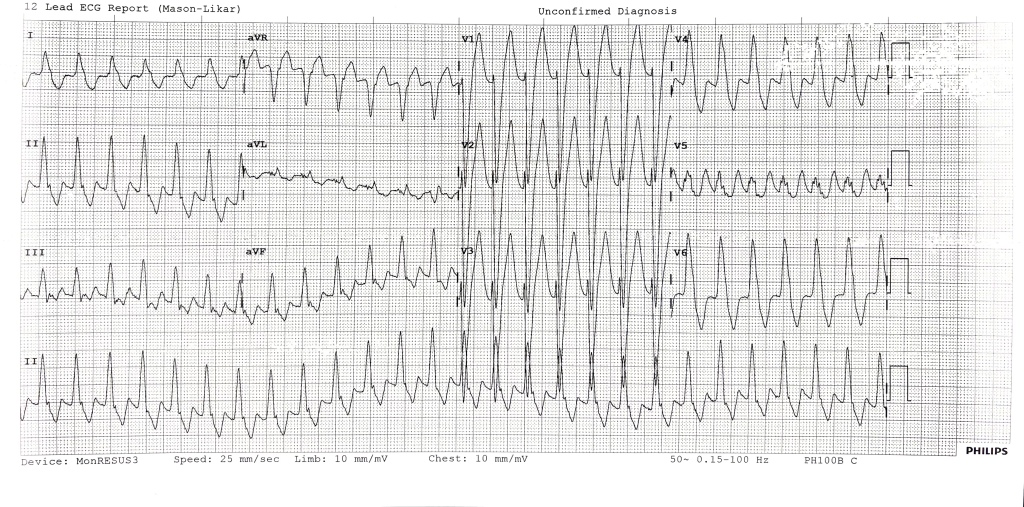
This young patient walked in to ED with palpitations.
Describe and interpret this ecg
This 12 lead ECG shows a regular broad complex tachycardia ~170bpm with an undulating baseline. Axis is normal and there are no obvious fusion or capture beats. There is no universal concordance.
Josephson sign is negative, but the R-S interval appears >100ms in V4-6.
There are some features both for and against VT in this case. As ever, if in doubt treat as for VT.
The patient underwent a successful DCR.
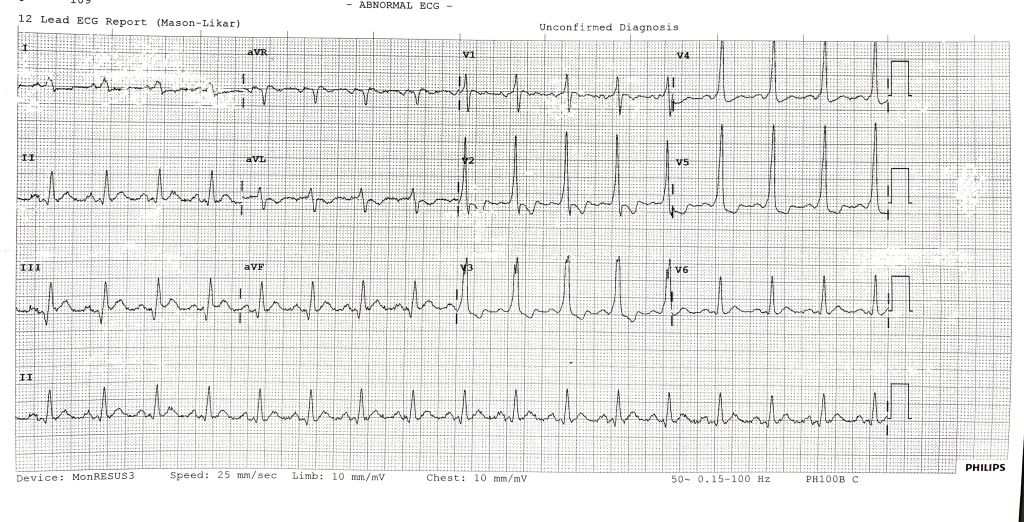
Describe and interpret this second ecg
This ECG shows SR rate of 90, with short PR interval, wide QRS and delta waves. There are discordant ST segments and T waves and an rSR pattern anteriorly.
These findings appear very characteristic of Wolf-Parkinson White Syndrome.
WPW is a syndrome associated with an accessory pathway in the heart which bypasses the AV node. Is is associated with tachyarrhythmias (usually AF and AFlutter and Atrio-ventricular re-entry tachycardia, AVRT). VT can occur but is rare.
In this case there is likely AVRT with antidromic (retrograde) conduction down the accessory pathway causing a wide complex tachycardia difficult to distinguish from VT.
In stable patients drug therapy can be considered, avoiding adenosine but again, should be treated as VT if concerned.
Visit the links below for more detail on this topic:
Cheers,
James

Leave a comment