Describe and interpret this ecg
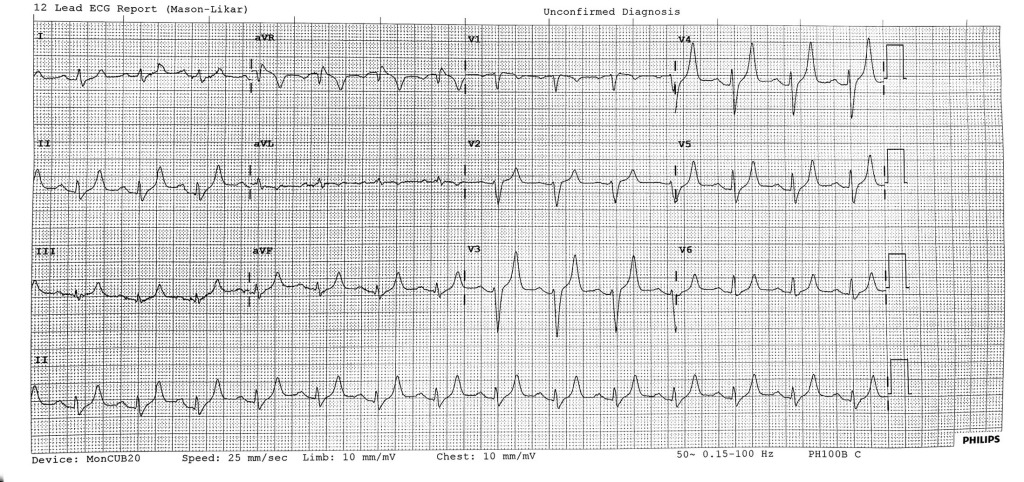
This 12 lead ECG shows 1st degree AV block with PR 200ms at a rate of 84bpm.
The axis is normal.
The striking abnormality is extremely tall, narrow, symmetrically peaked T waves visible throughout all leads.
There is a suggestion of P-wave flattening and the QRS duration is borderline at ~120ms.
There are always other possibilities for any given finding, but these findings appear very characteristic of hyperkalaemia.
Hyperkalaemia typically causes bradyarrhythmias and AV block, and new slow AF is particularly characteristic.
What is the treatment?
This patient should be immediately moved to resus and full cardiovascular monitoring initiated. They should be assessed for symptoms of presyncope, renal failure and a medication history taken. Concurrently without delay they should be given iv calcium (eg 10ml 10% calcium gluconate stat) to stabilise the myocardium. Hypertonic saline would also be an effective choice. This buys time for the next steps to work.
Next measures should be taken to reduce the blood potassium level. This can be done by redistribution – insulin dextrose infusion (10u actrapid in 50ml 50% dextrose over 30mins) and/or salbutamol (eg 5mg nebulised).
Elimination is achieved via the kidney (though loop diuretics like frusemide, or via isotonic HCO3 administration), bowel (calium resonium) or via haemodialysis. Haemodialysis particularly should be considered early in renal failure patients, severe hyperkalaemia (K+ >7 or haemodynamic compromise) or those worsening despite treatment.
This patient had acute on chronic renal failure and was found to have a K+ of 9.2 on the formal bloods.
This table from EMCRIT summarises these treatments


Leave a reply to edichan18 Cancel reply